
25th March 2001
News/Comment|
Editorial/Opinion| Business|
Sports| Mirror Magazine

Bring on the colonoscope
By Chris Fernando
Q: I am a 50-year-old male. Recently, I noticed that I had passed a fair quantity of blood with my stools. I discussed this with my family doctor who referred me to a specialist to have a colonoscopy done. I am a bit apprehensive as to what would be found as this test sounds rather serious. What exactly is a colonoscopy and what can it find?
Dr. Maiya says:
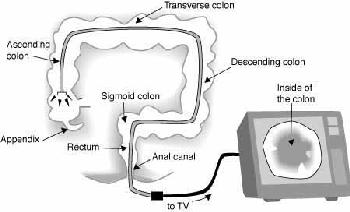
A colonoscopy is performed with the colonoscope, which is a very flexible fibreoptic scope over one metre in length and about the girth of an adult index finger.
This procedure is carried out under sedation and is very painless. Through this test, the entire large bowel and colon, which is obviously the site of the bleeding, can be viewed via a TV screen. This is called a video endoscope, which is now available in most hospitals both private and government.
Before a colonoscopy can be performed, the large bowel has to be cleaned of all faecal matter. Therefore, a laxative is prescribed before the test is performed .
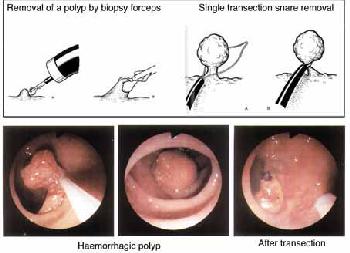
The most important thing about a colonoscope is that, in addition to being able to observe the offending lesion, therapeutic and diagnostic procedures can also be performed. These involve the removal of pieces of a probable growth for histological examination and also the complete removal of a polyp, which is an outgrowth of the inner lining, which may subsequently give rise to a cancer. In the past, before the invention of the colonoscope, polyps had to be removed by open surgery.
 Therefore,
the colonoscope is a major breakthrough in medical science since a diagnosis
can easily and accurately be made and pieces of tissue can be removed for
further examination and in addition, curative procedures such as the removal
of polyps can be carried out
Therefore,
the colonoscope is a major breakthrough in medical science since a diagnosis
can easily and accurately be made and pieces of tissue can be removed for
further examination and in addition, curative procedures such as the removal
of polyps can be carried out
It would be good to perform a colonoscopy in your case as bleeding with stools could be due to one of several causes, the most common being haemorrhoids, which are commonly called internal piles. These are situated within a couple of centimetres of the anal verge in the anal canal. So as we insert the colonoscope into the anal canal, the piles will become visible and depending on the size of these piles, injections or surgery can be decided upon.
When you insert the colonoscope further, it enters the rectum, which can harbour a polyp from which you can have bleeding. If so, it can be completely removed by passing a snare through the colonospe. The polyp is strangulated by the snare and burnt by a diathermy current. If we spot a large growth, which can occur in any part of the large bowel, pieces can be removed for further examination.
 We
might even see a diffused involvement of the entire inner lining which
is characteristic of an inflammatory bowel disease called ulcerative colitis.
In order to confirm the diagnosis, we have to take pieces for biopsies.
This can easily be done through the colonoscope. This disease can affect
any part of the large bowel and can produce blood and mucous in stools.
Another condition is Diverticulosis, which mainly affects the sigmoid colon
situated beyond the rectum.
We
might even see a diffused involvement of the entire inner lining which
is characteristic of an inflammatory bowel disease called ulcerative colitis.
In order to confirm the diagnosis, we have to take pieces for biopsies.
This can easily be done through the colonoscope. This disease can affect
any part of the large bowel and can produce blood and mucous in stools.
Another condition is Diverticulosis, which mainly affects the sigmoid colon
situated beyond the rectum.
Diverticulosis is a very common disorder where pockets develop in the colon because of increased colon pressure and spasms. These pockets are lined with only the inner lining of the gut. So through the colonoscope, you will see small blind-ended multiple holes in the colon and these can be the seats of infection. Once infection sets in, bleeding can take place or the entire area can get infected and convert the normally very flexible sigmoid colon into a rigid tube. Beyond this area, the colonoscope enters the descending colon, travels down to the ascending colon and to the caecum where the appendix originates and the small bowel terminates.
One other condition of inflammatory bowel disease is Crohn's Disease,
which also gives a granular appearance to the inner lining. However, biopsies
will have to be performed for further diagnosis. Sometimes, there could
be areas in the mucosa affected by micro vascular abnormalities, which
produce torrential bleeding that stops spontaneously. These can also be
seen via the colonoseope and surgical measures will be required if this
bleeding continues. So as you can see, with a colonoscope you can not only
arrive at a diagnosis, but also perform therapeutic procedures.
Cholesterol - the good and the bad
Cholesterol is a soft, waxy substance found among the lipids (fats) in the bloodstream and in all the body's cells. It is normal to have cholesterol. It's an important part of a healthy body because it's used to form cell membranes, some hormones and other needed tissues. But too high a level of cholesterol in the blood is a major risk factor in coronary heart disease, which leads to heart attacks.Hypercholesterolemia is the term for high levels of blood cholesterol. Cholesterol is made in two ways. The body makes some of it, and the rest comes from animal products that are eaten, such as meats, poultry, fish, eggs, butter, cheese and whole milk. Food from plants like fruits, vegetables and cereals do not have cholesterol. Cholesterol and other fats can't dissolve in the blood. They have to be transported to and from the cells by special carriers called lipoproteins and there are two kinds that one needs to be concerned with. Low-density lipoprotein, or LDL, is known as "bad" cholesterol. High-density lipoprotein, or HDL, is known as "good" cholesterol. The body makes HDL cholesterol for its protection. Studies suggest that high levels of HDL cholesterol reduce the risk of a heart attack.
Why is LDL cholesterol "bad"?
When too much LDL cholesterol circulates in the blood, it can slowly build up in the walls of the arteries that feed the heart and brain. Together with other substances it can form plaque, a thick, hard deposit that can clog those arteries. This condition is known as atherosclerosis. If a clot (thrombus) forms where a plaque is, the blood flow can be blocked to part of the heart muscle, causing a heart attack. If a clot blocks blood flow to a part of the brain, a stroke results.
Why is HDL cholesterol "good"?
It is believed that HDL tends to carry cholesterol away from the arteries and back to the liver, where it is passed from the body. Some experts believe that excess cholesterol is removed from atherosclerotic plaques by HDL, thus slowing the build-up. However, low HDL cholesterol levels may result in a greater risk of heart disease.
What is the triglyceride connection?
Triglyceride is a form of fat. It comes from food and is also made in the body. People with high triglycerides often have a high total cholesterol, a high LDL cholesterol and a low HDL cholesterol level. Many people with heart disease also have high triglyceride levels. Several clinical studies have shown that people with above-normal triglyceride levels have an increased risk of heart disease. Doctors need to treat high triglycerides in people who also have high LDL cholesterol levels. People with diabetes or who are obese are likely to have high triglycerides.
What is the 'ideal' blood cholesterol level?
Your total blood cholesterol will fall into one of these categories: Desirable less than 200 mg/dL. Borderline high risk 200-239 mg/dL. High risk 240 mg/dL and over
Desirable - If your total cholesterol is less than 200 mg/dL, your heart attack risk is relatively low, unless you have other risk factors. Even with a low risk, it's still smart to eat foods low in saturated fat and cholesterol, as well as get plenty of physical activity. Have your cholesterol levels measured every five years or more often if you're a man over 45 or a woman over 55.
Borderline high risk - In general, people who have a total cholesterol level of 240 mg/dL have twice the risk of heart attack as people who have a cholesterol level of 200 mg/dL.
Have your cholesterol and HDL rechecked in one to two years if: *Your total cholesterol is in this range. *Your HDL is less than 35 mg/dL. *You don't have other risk factors for heart disease. Nevertheless, ask your doctor to interpret your results. Everyone's case is different.
High risk - If your total cholesterol level is 240 or more, it's definitely
high. Your risk of heart attack and, indirectly, of stroke is greater.
Ask your doctor for advice.
Cataract and an eye for an eye!
A cataract is a clouding of the part of the eye known as the crystalline lens. The lens is a clear tissue located behind the pupil. The lens works together with the transparent cornea, which covers the eye's surface, to focus light on the retina at the back of the eye. When the lens becomes cloudy, or cataractous, light cannot pass to the retina properly, and vision is blurred and decreased.Although cataracts result from many conditions, the most frequent cause is the natural aging process. Other causes may include injury, chronic eye disease and other system-wide diseases such as diabetes. Cataracts can take from a few months to several years to develop. Sometimes, the cataract stops developing in its early stages and vision is only slightly decreased. But if it continues to develop, vision is impaired, and treatment is necessary.
Surgery to remove the diseased lens is the only effective treatment for cataract. And in the majority of those cases, the diseased tissue is replaced with an artificial device known as an intra-ocular lens implant. In a cataract operation, the eye's natural lens is removed. A new lens replaces the removed one for vision to be restored. This new lens can be in the form of special eyeglasses with thick lenses or contact lenses. Most commonly, it is in the form of an intra-ocular lens implant.
The artificial lens is made of plastic and is usually inserted at the
same time the cataract is removed. Depending on the individual case, the
lens is placed directly behind or, less frequently, in front of the iris.
Not every case is appropriate for this type of procedure, and the method
of implantation used depends on the individual. Once the surgeon has determined
that intra-ocular lens replacement is appropriate, the patient undergoes
a special preoperative evaluation. Like contact lenses and "prescription"
eyeglasses, intra-ocular lenses differ in terms of refractive power, and
the evaluation determines the proper lens power of the implant. The natural
lens has the ability to accommodate, or change shape, so that it is possible
to focus at varying distances. The intra-ocular lens, which cannot change
shape, is usually calculated for a middle distance so that the patient
can see well enough to move about without glasses. Normal eyeglasses must
still be worn to see close up and far away. In most cases, though, patients
notice significant improvements in vision resulting from intra-ocular lens
implantation. Generally, cataract surgery lasts about an hour and is usually
performed on an outpatient basis. In some cases where there is a previously
existing medical problem or when advised by the surgeon, hospitalization
may be needed. Because of inflammation related to the surgery, initial
vision may remain cloudy for a few days or weeks. Clear vision generally
returns in about three months.
Accident Service celebrates ten years in new premises
It's no accident
By Hiranthi Fernando
The Accident Service of the Colombo National Hospital celebrated 10 years in its new premises on March 15. The building and equipment which cost Rs 750 million was a gift from the Government of Finland.Improving the Accident Service was one of the aims of the Colombo General Hospital rehabilitation project, Director of the National Hospital, Dr. Hector Weerasinghe said.
The first Accident Service was established in 1965 in the Victoria Memorial Building, which was formerly the Eye Hospital. "This building was very small and had facilities only for about 65 patients," Dr. Weerasinghe said. "There was only one operating theatre and patients had to be admitted to General Surgical wards since there were insufficient Orthopaedic beds. So there was an urgent need for improvement."
The new Accident Service has a spacious Out Patients Department (OPD), seven operating theatres and seven wards with beds for 260 patients. It is also equipped with a central sterile supply department and two intensive care units, one for general surgical cases and one for neuro-surgery. "It made a significant improvement to our services," Dr. Weerasinghe said. "The staff of the Accident Service were originally trained by Finnish consultants and a team from Finland worked here for the first year."
"During the last ten years, we have treated one million patients with injuries, at the Accident Service," Dr. Weerasinghe continued. Each day an average of 300 people injured in road accidents, domestic and industrial accidents, sports, and all forms of violence are treated at the Accident Service. "Violence is a major component of the injuries today," added Dr. Weerasinghe.
Commenting on the improvement in the service given to the public, Dr. Weerasinghe said that in 1990, about 80,000 patients were treated at the old Accident Service unit, while today the average is 100,000 to 120,000 patients a year. Admissions which were around 19,000 a year in 1990 have increased to 25,000 and as for the surgical procedures performed, 10,000 in 1990 have doubled in the last ten years.
The Accident Service has a staff of around 600. During the last ten years, they have had to cope with about 25 disasters. "The first was the bomb blast at the JOC Headquarters, where we treated about 200 to 300 victims," Dr. Weerasinghe recalled. "The biggest however was the Central Bank bomb blast, when 1500 were brought for treatment in one day. During the last year, there were eleven disasters the Accident Service has had to cope with.
Dr. Weerasinghe said the Accident Service also has a 'disaster store' of medical supplies. As part of their disaster plan they have four teams, one of which is on call for the Accident Service each day. When it is a minor disaster, the team on call rushes in but when a major disaster strikes, all the teams rush to the hospital to assist. "We alert blood banks, ICUs, and operating theatres to be ready for an emergency. In this country, when there is a disaster, we have found that the public on their own, volunteer and queue up to donate blood."
The experience the staff of the Accident Service has had in managing major disasters, has been recognized in the region. Three WHO sponsored workshops have been held in Colombo for nursing staff of the SAARC region. Severe overcrowding is one of the major problems they have. "When the new building came up, we thought we could manage, but the numbers are so big," the Director said.
The solution, he feels is not to expand further in Colombo but to improve the periphery. Accident Services should be established in major towns like Kandy and Galle, he says.







![]()
Front Page| News/Comment| Editorial/Opinion| Plus| Business| Sports| Mirror Magazine
Please send your comments and suggestions on this web site to