Our lungs enable us to breathe, the vital function essential for life. They can be described as sacs of air which are located inside a confined space called the chest cavity. They are suspended in the chest cavity and separated from the chest wall by a small thin space called the pleural cavity. The normal functioning of the lungs is a complex mechanism and a small fault in this can cause a life-threatening condition.
A pneumothorax is an unwanted collection of air in your chest cavity (pleural cavity) between the lung and the chest wall. This can occur spontaneously in young adults and is called Primary Spontaneous Pneumothorax (PSP). PSP is common in young males rather than in females. Its incidence in the general population is 18/100,000 in males and 6/100,000 in females per year. It happens most commonly between the ages of 20 and 40. As this is a life threatening condition early recognition and treatment is essential.
What happens if you have
a pneumothorax?
If the air gets trapped in the chest cavity outside the lung (in the pleural cavity), there will be specific problems arising due to the pressure effect caused by this air. The lungs are like sponges, filled with air and if the air keeps collecting in the chest cavity outside the lung, the lung can no longer expand normally. Lung tissue gets squeezed just like a sponge. Therefore it cannot take up adequate air required for our body to function.
Luckily, we have two lungs which are in two separate cavities without any communication between the two cavities (unlike in some mammals). This provides a safety mechanism as the lung not affected can compensate for a period before everything fails.
What causes spontaneous
pneumothorax (PSP)?
A primary spontaneous pneumothorax is caused by a leak in the lung surface, which causes air to leak outside the lung into the chest cavity. Individuals with PSP do not have any underlying lung disease. But 60% of the CT scans carried out on these patients shows underlying blebs or small bullaes in the upper most parts of the lungs. These blebs are small air-filled sacs on the surface of the lungs which have a thin wall, which can easily burst. The air leak is caused due to rupture of these thin walled air sacs. Apart from these blebs having the risk of popping and causing a pneumothorax they do not cause any other long standing lung disease or predispose them to any.
There are also pneumothoraces which can be caused by other lung conditions, this is called secondary pneumothorax. Trauma, a pre-existing lung condition and tumours of the lungs can cause these.
What are the symptoms?
- Sudden onset single sided chest pain-may be a mild discomfort or severe
- Difficulty in breathing
Symptoms are proportional to the size of the pneumothorax and the individual’s lung reserves (fit and healthy athletic individuals have good pulmonary reserves). In any case sudden onset symptoms should prompt a visit to the doctor and if you have severe symptoms it is an emergency requiring immediate admission to hospital.
A minority of people can develop a live threatening condition which is called a “tension pneumothorax’’. A Tension Pneumothorax is due to severe air leak causing compression of lungs and heart in the confines of the chest cavity.
Although a primary spontaneous pneumothorax rarely results in death, developing tension pneumothorax can lead to death. It is an emergency which requires immediate release of air from the chest cavity.
What must we do?
If a young adult develops sudden onset chest pain or difficulty in breathing, he or she must be seen by a medical practitioner and a chest x-ray should be taken to exclude a pneumothorax. (Your medical practitioner is qualified to assess the symptoms and decide on a chest x-ray).
Depending on the severity of the symptoms the medical practitioner can decide whether to admit directly or assess the chest x-ray before admitting. When it is a small pneumothorax, it not is apparent on a chest x-ray and the patient may require further investigating with a CT scan which is more sensitive. If further treatment is required a CT will provide all the information required for the management of the pneumothorax. It also enables the clinician to identify the cause of the pneumothorax.
What is the management?
Primary spontaneous pneumothorax is a recurring disease and it can affect both lungs, causing damage to a normal lung, if left untreated. Treatment options can be divided into emergency treatment and definitive treatment
Emergency treatment
Almost all cases of pneumothorax require admission to a hospital. Treatment depends on the severity of the pneumothorax on the chest x-ray and severity of the symptoms.
In most people, symptoms improve within 24 hours. With time, collected air inside the chest cavity may get absorbed and the condition improves.
Observing the patient
Patients with minimal symptoms and a small pneumothorax on the chest x-ray can be observed in an emergency treatment unit without admission. A chest x-ray will be repeated to check if the size of the pneumothorax is reducing. If it has significantly reduced in size, the patient will be able to go home. However, the patient should be seen and assessed by a chest physician at a later date.
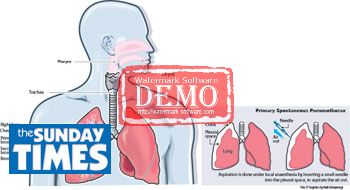
Aspirating the pneumothorax
If the pneumothorax is small and the patient is symptomatic, a medical practitioner may decide to aspirate the pneumothorax to remove the air out from the chest cavity. This is done after admitting the patient to the hospital or in the emergency department of the hospital. Aspiration is done under local anaesthesia by inserting a small needle into the pleural space, to aspirate the air out. This is generally well tolerated.
Intercostal tube insertion (Chest Drain)
If the pneumothorax is moderate to severe and the patient has moderate to severe symptoms, then the patient requires an intercostal tube insertion whilst in hospital. This is carried out by a trained medical officer under local anaesthesia.
A small calibre tube is inserted to the patient's affected chest cavity to get the air out. One end of the tube stays inside the chest cavity and the free end is connected to specially made bottle filled with water.
Once the intercostal tube is inserted, the patient must stay in the hospital till the removal of the tube. This can be between 3 -10 days. The tube normally stops bubbling when the air in the chest cavity (the pleural space) has all come out.
Whilst the tube is inside, repeat x-rays will be taken to assess the size of the pneumothorax. If all is well the tube is removed and the patient will then be discharged.
The most important thing to remember is that primary spontaneous pneumothorax (PSP) is a recurring condition.
If a person develops a single episode, there is a 30% chance of him having another pneumothorax in the same side and there is a 10% chance of him having a pneumothorax in the opposite side. After the second attack, the chance of developing a third attack is as high as in the range of 40-50%. Most recurrences occur within the first two years of the first episode. Therefore the patient should be referred for follow-up by a chest physician or a Thoracic surgeon.
Importantly, prior to the patient being discharged, the patient should be warned regarding the risk of recurrence.
What to do once you go home following
pneumothorax
- Avoid air travel until a chest radiograph has confirmed resolution of the pneumothorax. (Medical advice is needed before planning air travel)
- Diving should be permanently avoided after a pneumothorax, unless the patient has had both sides corrected by surgical operations.
- Primary pneumothorax patients who have not undergone definitive surgical treatment must avoid activities where emergency medical care is not available E.g. being on fishing boats (trawlers), long air travel, travelling in places where there is no access to emergency care (jungle hiking, mountain climbing)
Other sports activities and exercises should be encouraged. Exercises including surface swimming (swimming pools, or in a safe environment) will increase the lung capacity and should be encouraged.
All patients discharged after active treatment or otherwise should be given verbal and written advice to return to the Accident and Emergency Department immediately should they develop further breathlessness.
Definitive treatment
All patients with pneumothorax should be referred to and must be seen by a respiratory/ chest medicine team--Chest Physician/Thoracic Surgeon) to exclude secondary causes for pneumothorax (secondary Pneumothorax due to existing lung disease is different from primary spontaneous pneumothorax PSP) and for definitive treatment.
Need for definitive treatment will be decided by the respiratory/ chest medicine team after the patient assessment is complete.Definitive treatment can be Chemical pleurodesis or surgical pleurodesis.
Chemical pleurodesis
This is done with introduction of chemically irritant agents through the chest drain into the chest cavity. Recurrence of attacks is significantly reduced. The chance of recurrence is about 15%.
Problems associated with chemical pleurodesis are:
1.Severe intense chest pain
2.Vaso-vagal attacks
3.It does not reduce the hospital stay compared to surgical options.
4.Recurrence rate is 15%, and when recurrences occur, subsequent surgery is difficult
Surgical pleurodesis
The aim of surgical pleurodesis is to identify and remove the small air filled sacks (blebs) which causes pneumothorax and to obliterate the space between the lung and the chest wall by making the lung glued to the chest wall. The recurrence rate following surgical pleurodesis is 1%. (Statistics-Chest Hospital Welisara). Surgical pleurodesis is carried out under general anaesthesia. It can be done by an open operation (mini Thoracotomy-with 4-5cm skin incision) or as Video assisted Thoracoscopic operation with 2cm small two skin incisions.
There is no significant difference in recurrence rate or hospital stay between open and video assisted operations. The major difference between the two methods is the time taken to complete the operation and a small scar when video assisted surgery is performed The open operation takes about 2 hrs to complete while the video assisted operation only takes about 30 -45 minutes.
Hospital stay when compared for open operation/video assisted operation or chemical pleurodesis remains the same e.g. 5-7 days. Surgical pleurodesis carries a very low recurrence rate (1-2%) and can be carried out safely. Complications following surgery for primary spontaneous pneumothorax are extremely low.
Surgical pleurectomy: Good results at Chest Hospital
The Thoracic Surgical Unit at the Chest Hospital Welisara has been performing Video Assisted Thoracoscopic Surgery (VATS) for pneumothorax since 2007, with over 100 procedures without any major complications and with minimal minor complications. Recurrence rate is around 1%.
Surgical pleurectomy is the most effective treatment available for Primary Spontaneous Pneumothorax (PSP) and can be carried out safely with minimal complications.
(The writer is a Consultant Thoracic Surgeon) |