Jaundice refers to the yellow appearance of the skin and whites of the eye that occurs when the blood contains an excess of the pigment called bilirubin.
Bilirubin is a natural product arising from the normal breakdown of red blood cells in the body and is excreted in the bile, through the actions of the liver.
Although jaundice is most often the result of a disorder affecting the liver, it can be caused by a variety of other conditions affecting, for example, the blood or spleen. It should be thoroughly investigated, so that the underlying cause can be identified and treated.
How do you get jaundice?
The red blood cells in our circulation carry oxygen to all parts of the body and have a life span of about 120 days. At the end of their life, they are broken down and removed from the circulation by special cells called phagocytes, which are found within the bone marrow, spleen and liver.
New red blood cells are of course continually manufactured, and this also takes place within the bone marrow.
Following the breakdown of the red blood cells some of their component parts – such as amino acids and iron – can be re-used by the body. Other components such as bilirubin need to be removed.
Knowing how this removal pathway works is the key to understanding how jaundice occurs.
Most waste products of the body are excreted in the urine via the kidneys, but the liver and bile system is the other main physical route out of the body for these substances. By ‘waste products’, we mean the many compounds that arise in the course of the body’s metabolism. But almost all forms of drugs must also be eliminated either via the urine or bile routes.
In the case of bilirubin released from old red blood cells, it passes through the bloodstream to the liver, where the liver cells process it.
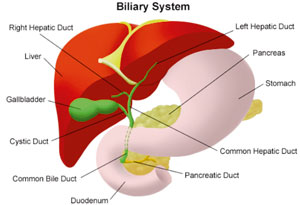
These cells carry out many complex chemical functions and also produce the liquid bile that is the ‘vehicle’ by which the cells discharge their output to the bile duct system. This is a branching network of tiny tubes throughout the liver that merge in the same way as the branches of a tree.
Ultimately, a single main bile duct comes out of the liver and joins the first part of the small intestine (duodenum). Bile (and therefore bilirubin) then passes out through the small and large intestines and is excreted in the stool (faeces).
Bile is green in colour. But bacteria in the large bowel act to change the bilirubin to substances that are brown, which gives stool its characteristic colour. Some of the bilirubin is reabsorbed back into the body through the bowel wall – eventually appearing in the urine as a substance called urobilinogen.
Therefore, any failure of the bilirubin removal pathway will lead to a build-up of bilirubin in the blood. When this happens the individual’s skin turns yellow – causing jaundice.
What conditions can be
associated with jaundice?
An excessive breakdown of red blood cells:
The manufacture and breakdown of red blood cells is normally precisely balanced and equal. But there are several conditions in which the rate of breakdown increases. If the amount of bilirubin released exceeds the liver’s capacity to remove it – jaundice will develop.
The medical term for excessive red cell breakdown is ‘haemolysis’. Malaria is an example where the parasites live within the red blood cells and shorten their life.
Similarly, is the condition in which a foetus develops haemolysis, due to incompatibility of its Rhesus blood group with that of its mother.
Autoimmune haemolytic anaemia is a rare disease in which the body’s immune system seems to attack the red cells. It usually affects adults.
Haemolysis can also be a side-effect of some drugs.
Impairment of liver function:
The commonest cause is a viral infection of the liver cells (hepatitis). Many different types of infection including glandular fever (mononucleosis) can also be responsible for this.
Alcohol abuse and subsequent scarring of the liver (cirrhosis) can cause significant cell damage leading to jaundice.
Other less common conditions causing liver cell damage include:
- Non-alcoholic steatohepatitis or NASH (a condition in which fat and scar tissue accumulate in the liver)
- Hemochromatosis (a condition in which there is too much iron in the body)
- Autoimmune hepatitis (a condition in which the body’s immune system recognises the liver as foreign)
- Wilson’s disease (a rare disease of copper metabolism)
- Tumours of the liver – either primary liver cancers (arising from the liver tissue itself) or more commonly, the secondary spread of a tumour from elsewhere in the body into the liver – can lead to cell failure and jaundice.
Blockage of the bile ducts:This can occur as a result of abnormality inside or outside the ducts. The commonest example of an internal blockage is a gallstone.
Tumours of the bile duct are rare. But if large enough, or situated just where the bile duct meets the duodenum, then they can block the flow of bile.
At this junction point, known as the ampulla of Vater, the tube from the pancreas gland also joins the duodenum. Cancer of the pancreas tends to arise in the part of the pancreas nearest to the ampulla of Vater, so is another potential cause of ‘obstructive’ jaundice.
Any external organ or mass lying nearby that becomes large enough to press on the bile duct could be responsible.
Examples include: swollen internal lymph glands, a cyst (perhaps of the pancreas) or scar tissue following a previous infection or surgery.
What are the symptoms?
The symptoms, other than that of the jaundice itself, will relate to the underlying cause.
For example, someone with haemolysis might also be anaemic and tired.
If a gallstone were responsible, there would probably have been a preceding history of pain in the abdomen. A cancer might be accompanied by weight loss and other symptoms.
When jaundice is due to obstruction of the bile duct, the person will often notice that their urine becomes dark and stools become pale because the excess bilirubin ‘spills over’ into the urine and no longer colours the stool.
Obstructive jaundice is also often accompanied by intense itching.
How is jaundice diagnosed?
The diagnosis is made by recognition of the patient’s appearance and accompanying symptoms.
A blood test will confirm the raised bilirubin level and other tests, such as those for hepatitis and haemolysis, are also done on the blood.
Ultrasound is a good way to inspect the liver and bile ducts for signs of obstruction and often can give useful information on the pancreas gland.
CT or MRI scanning also helps diagnose obstructive jaundice accurately.
What can your doctor do?
If you suspect that you may have jaundice, see your doctor so that the underlying cause is identified and treatment initiated as soon as possible.
Treatment will depend upon the diagnosis. For example, if the problem is one of gallstones, removal of the gallbladder may be required.
(The writer is a Consultant Physician, Gastroenterologist & Hepatologist) |