The abnormal accumulation of a water-like substance called cerebrospinal fluid in the brain is called hydrocephalus. The word Hydrocephalus comes from the Greek 'hydro' meaning water and 'cephalus' meaning head.
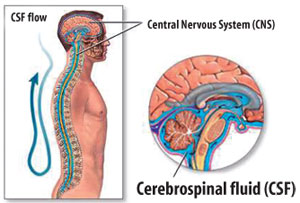
Cerebrospinal fluid (CSF) is made in the brain ventricles or cavities. The circulation of CSF in the brain and spinal cord and around it provides a cushioning effect that protects these delicate structures. It also maintains the balance of nutrients to these tissues and takes away the waste products produced.
The delicate balance achieved by the production and absorption of CSF can be altered due to certain conditions and when this happens excess production or under absorption may occur, resulting in hydrocephalus.
Developing hydrocephalus normally increases the pressure in the head. This may give rise to symptoms such as headaches, vomiting and visual disturbances. Hydrocephalus can be congenital (from birth) or acquired (after birth). Today MediScene looks at the condition called normal pressure hydrocephalus.
Normal Pressure Hydrocephalus (NPH)
This is an acquired condition and as the name suggests, unlike other hydrocephalus the pressure may be 'normal'. This is probably due to the fact that the accumulation of CSF occurs slowly over time. This allows the brain to adapt to the increase in pressure. The slow enlargement of the fluid containing cavities means that the fluid pressure in the brain may not be as high as in other types of hydrocephalus. But the enlarged cavities still press on the brain and therefore can cause symptoms. The condition is becoming recognized more often now.
Causes
In some patients a cause is identified, for example a previous bleed in the brain or a tumour blocking the CSF pathways. But in most the cause of NPH is unknown.
Incidence
This condition is still rare (or it could be that it is under diagnosed). The incidence internationally is thought to be 1 case per 25,000 of dementia patients. It affects males and females equally. The age of presentation is greater than 60 years.
Symptoms
There is an identified triad of classic symptoms
1. Progressively worsening memory loss
2. Progressively worsening problems with walking
3. Problems with bladder control and incontinence
Diagnosis
The patient should be seen by a doctor who is able to record his/her history and conduct a thorough examination. The patient should be accompanied by a family member who can give the full history regarding the progression of symptoms. The main aim is to rule out other causes of memory impairment, for example other dementias such as Alzheimer's disease and vascular dementia
Routine blood tests are also carried out to rule out any other underlying conditions. The doctor will then refer the patient to either a neurologist or a neurosurgeon for further assessment and investigations.
Investigations
The first investigation to be carried out will be a CT or MRI scan. This enables the doctor to ascertain whether there is an increase in the size of the cavities in the brain with CSF- Hydrocephalus. The scans also enable other conditions such as tumours to be ruled out. More sophisticated MRI scans which allow you to look at the flow of CSF through the brain may also be useful and maybe requested if available.
If there is no structural obstruction to the flow identified then the patient undergoes a barrage of investigations.
The patients walking will be assessed and documented, for instance how many steps he or she can walk in a given time. The memory impairment will be assessed and noted. The patient may then undergo a lumbar puncture (please see box) where CSF fluid is taken out and the pressure within the head is also measured. Some fluid is removed after which the tests are repeated. If the symptoms improve, this gives the doctor some indication that the patient's symptoms may improve with the permanent drainage of excess CSF.
Treatment
If the results indicate that after drainage of excess CSF the patient improves then there is a surgical option of placing a shunt to drain this fluid. A ventriculoperitoneal shunt is placed by a neurosurgeon. This device drains the excess CSF from the brain cavities into the abdominal cavity. This involves surgery and is a permanent device - success is only seen in a small percentage of patients. It is essential that thorough communication takes place between the surgeon, patient and family regarding the risks and benefits.
The main aim of this article is to create awareness that such a condition exists and that treatment is also available. Not all patients will have clear cut symptoms and it is essential that other dementias are ruled out. There is still a great degree of research being carried out throughout the world looking into this condition and the best way to treat it.
Shuffling, stooped walking
In the classic triad the walking problems precede the others. The patient takes wide based, short shuffling steps. He/ she would normally have difficulty in turning suddenly. Patients often feel that they are 'stuck to the ground', and have difficulty in initiating steps or turns. The memory impairment is noted with associated slowness of thinking.
The urinary incontinence is usually unwitting and maybe associated with memory impairment and difficulty in getting to the toilet quick enough.
A Lumbar Puncture
This is a test carried out by a doctor to test the cerebrospinal fluid which circulates around the brain and the spinal cord. It is done to check for infection - for example when diagnosing meningitis, to check the pressure within the brain and also to detect cancer cells.
It is carried out in the ward with the doctor explaining the procedure to you.
The doctor will need to put a needle into your spine to collect some fluid that drains out. You will have to lie on your side and curl up, bringing your knees to your chest. This allows your back to curve towards the doctor. You need to be comfortable.
The doctor will expose your lower back and then place on sterile gloves and cloths over you to keep a sterile area and thereby prevent infection from entering the spinal fluid. A small amount of local anaesthesia will be injected to numb the area which will be cleaned with antiseptic solution; this time also allows the anaesthesia to work.
When ready the doctor will push a needle very carefully into the small of your back. You should be able to feel the pushing sensation but not unbearable pain. Tell the doctor if you do feel significant pain.
The needle enters the space surrounding the lower part of the spinal cord. A drop of clear fluid indicates that the right space has been reached. The pressure is measured and then fluid is allowed to flow. The needle is then gently removed. The fluid is sent for analysis. A sterile dressing is applied and you will be advised to stay in bed for a while and to gradually get up to avoid a bad headache. |