
When narrowed vessel gets new lease of lifeIn our continuing series on common surgical procedures, Dr. Melanie Amarasooriya talks to Dr. Sepalika Mendis, Consultant Cardiologist, National Hospital Sri Lanka about coronary artery bypass grafting surgery When Mr. Perera, a 52-year-old bank executive, developed a tightening pain just under the breastbone in the central area of the chest, while walking uphill, he did not worry too much. He stopped to rest and the pain disappeared in a few minutes. Later on even gardening or walking a short distance would trigger this pain, though it would ease after he rested for a while. Since his father had had a heart attack, he grew anxious and consulted a doctor who ordered a few investigations saying the pain suggested 'ischemic heart disease' which meant, the blood vessels supplying the heart had narrowed due to deposition of cholesterol and hence the heart was not getting enough blood.
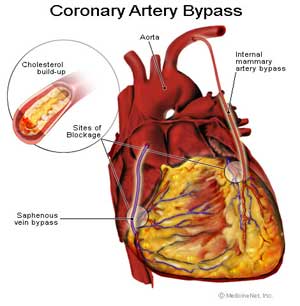
Mr. Perera's cholesterol level was high, but the resting ECG showed no changes. During the initial stage while the patient is resting, the heart may not show changes; only when the patient starts to exercise or exert, does the heart lack blood to meet with the increasing demand. An exercise ECG under supervision was ordered. It was strongly positive; his heart showed telltale signs that it did not get enough blood when he started to exercise. The next step was an angiogram, to assess the degree and the sites of narrowing of the vessels. Here a tube was placed in a blood vessel in the groin, through which a small, longer catheter was sent to the heart, injecting a dye into the vessels of the heart. With X ray screening, the blood vessels of Mr. Perera's heart were studied. A diagnosis of triple vessel disease was made. This meant the three major blood vessels that supply blood to the heart had narrowed due to deposition of cholesterol."Am I going to have a hear attack" was Mr. Perera's first question."Don't worry, It means just that your heart is not getting enough blood, so we have to correct that," the doctor said, adding that he may need coronary artery bypass grafting surgery. Mr. Perera was then referred to the cardiothoracic surgeon who performs 'by pass' surgeries. Coronary artery bypass grafting surgery is widely performed all over the world. This major surgery, lasting about 4 to 8 hours, involves taking a blood vessel from the patient's forearm, leg or other site and suturing it onto the heart, to bypass the narrowed segment. When there are several sites narrowed all those sites need to be bypassed with new vessels to establish blood supply to the heart. Mr. Perera was admitted to hospital for the operation. The doctor in the ward explained the procedure and got his consent. His blood group was A negative and blood was cross-matched and saved to be given when necessary. Surgery took about six hours and Mr. Perera was unconscious during the procedure. Immediately after, as he recovered from anaesthesia he was sent to the Intensive Care Unit for monitoring. There was a tube in his mouth accessing the respiratory passage, a catheter placed in his urinary passage, another plastic tube, a drain, on the chest, close to the site where the incision was done. There were other tubes in his blood vessels giving fluid, saline and medication. He was connected to the ECG monitor. Mrs. Perera was alarmed seeing her husband surrounded by wires and tubes. Beeping sounds from the monitors added to her fear. "Is he getting bad?" she asked the doctor in the ICU. "No, all patients after bypass surgery are admitted to the ICU for a brief period to monitor them closely for any problems that might arise. In more than 97 out of a hundred patients who undergo this procedure, the surgery goes as planned without any problem," the doctor explained. And of course, the patient was given medication for the problems that were already anticipated such as abnormal heart rhythms. After three days Mr. Perera was sent to the ward. The doctor explained how he needed to adjust his routine after the surgery. By about day 10 after the surgery Mr. Perera was feeling alright apart from a little soreness just over the chest wound. The doctors reassured him that it would go off in a few days. There was also a mild swelling in the leg from which the blood vessel for the surgery was taken. It was also examined; the wound was clean without any oozing or undue pain. Such mild swelling was normal after surgery. He was now fit to go home. But before discharge he was referred to the cardiac rehabilitation programme of the hospital to help him adapt his life. There he was educated about his illness, medication, and a tailor made exercise and diet plan was drawn up. He was also offered psychological support because he was feeling somewhat depressed after the illness. Now, three months on, he is back to normal, but sticks to a good exercise and diet plan, aware that the new vessels too can get narrowed by cholesterol deposition. It worked out very well for Mr. Perera. But prevention would have been far better.
|
|
||||||
|| Front
Page | News | Editorial | Columns | Sports | Plus | Financial
Times | International | Mirror | TV
Times | Funday
Times | Medi Scene || |
| |
Reproduction of articles permitted when used without any alterations to contents and the source. |
© Copyright
2008 | Wijeya
Newspapers Ltd.Colombo. Sri Lanka. All Rights Reserved. |