One of the most common symptoms of Gastro Esophageal Reflux Disease (GERD) is heartburn. That sensation has nothing to do with your heart - instead, it’s coming from your esophagus. A chronic digestive disease, the acid reflux that distinguishes GERD occurs when stomach acid or bile flows back into your food pipe. The backwash of acid inflames the lining – a sensation so uncomfortable it can keep you up all night.
For most people, dealing with heartburn is as simple as popping an antacid. But for people with GERD, this treatment offers only temporary relief. Stronger medications, even surgery, may be called for says Dr. Anuja Somaratne, Consultant Surgeon.
Keeping it down
Reflux can feel as unpleasant as it sounds. Sometimes coming from as far down as the duodenum (the first part of the small intestine that attaches to the stomach), the liquid contains acid and, on occasion, bile and pepsin (an enzyme that begins the digestion of protein in the stomach.) Of these, acid is considered the most injurious component.
Unfortunately, GERD is a chronic condition, though many experience it in cycles. An injury to the lining of the esophagus (esophagitis) though makes matters more serious, and can also recur once treatment is stopped. Your doctor will have to judge the severity of your case.
In the meantime, most reflux happens during the day, when an individual is upright and gravity will pull the refluxed liquid back in. Swallowing takes the liquid back into the stomach and the saliva that accompanies each swallow itself contains bicarbonate. The bicarbonate neutralizes the small amount of acid that remains in the esophagus. Reflux that occurs at night is more likely to result in acid remaining in the esophagus longer and causing greater damage to the esophagus.
What’s different?
While many people unconsciously have a reflux, in patients with GERD, the refluxed liquid can contain more acid, and the acid remains in the esophagus longer.
Certain conditions, such as pregnancy, increase a person’s vulnerability to GERD, as do diseases such as scleroderma that weaken the esophageal muscles.
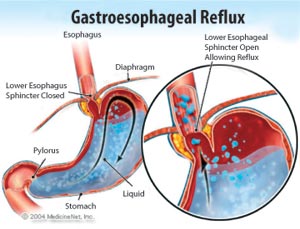
But all in all, the causes of GERD are complex. The proper functioning of the lower esophageal sphincter (LES) is perhaps the most crucial element when it comes to preventing reflux. This specialized ring of muscle contracts and closes off the passage from the esophagus into the stomach. Swallowing leads to the LES relaxing for a few seconds to allow the passage of food and then it closes again. In patients with GERD, abnormally weak contraction of the LES and abnormal relaxations of the LES allow reflux to occur more easily.
The act of swallowing itself triggers a contraction (peristalsis) that continues down to the lower esophagus. In patients with GERD, several abnormalities in this contraction have been observed. Smoking and alcohol both are known to increase acidity in the stomach. Hiatus hernias, a condition in which a small part of the upper stomach pushes up past the diaphragm, can also contribute to GERD. No longer at the level of the diaphragm, the LES is less effective.
What are the symptoms?
Heartburn, regurgitation, and nausea are the primary symptoms of GERD.
The first, usually described as a burning pain in the middle of the chest, may start high in the abdomen or may extend up into the neck and back. Some patients report a sharp pain that mimics angina (heart pain), rather than burning. As acid reflux is more common after meals, correspondingly, so is heartburn. Episodes of heartburn can be unpredictable, varying in intensity across weeks and months. Nevertheless, heartburn is a life-long problem, and it almost always returns.
Regurgitation is the appearance of refluxed liquid in the mouth. Nausea is uncommon in GERD. In some patients, however, it may be frequent or severe and may result in vomiting.
When things get complicated:
Long-standing, severe GERD causes changes in the cells that line the esophagus in some patients. These cells can become cancerous and demand careful monitoring.
In serious cases, acid reflux can wreak havoc, going deeply into the esophagus, and resulting in the formation of ulcers. These breaks in the lining of the esophagus occur in the inflamed area, and can be chronic in nature. In addition, as they heal, ulcers of the esophagus can leave behind scars, and over time these narrow the inner cavity of the esophagus. This scarred narrowing is called a stricture.
GERD has also been linked to sore throats and hoarseness, as well as inflammation and infection of the lungs. The last occurs because refluxed liquid has passed the larynx and entered the lungs. The reflux of liquid into the lungs (called aspiration) often results in coughing and choking and GERD is often suspected in cases of unexplained coughing. Travelling further, the fluid sometimes makes its way into the sinuses and middle ears, though this is most often seen in children.
Diagnosing and treating GERD:
Heartburn is the first indication that you have GERD. But it always pays to investigate thoroughly. Upper gastrointestinal endoscopy (also known as esophago-gastro-duodenoscopy or EGD) allows doctors a peek into what’s happening inside, but unless there’s inflammation or ulcers, there might not be something to see at that point.
Plus, ulcers aren’t a deciding factor. A type of infection called Helicobacter pylori, or even non-steroidal anti-inflammatory drugs have been known to cause ulcers and these conditions require that a different treatment regimen other than GERD’s be applied. In the end, esophageal acid testing is widely considered the most effective form of correctly diagnosing GERD. Here, an acid sensing device is used to measure how often the contents of the stomach reflux into the lower esophagus and how much acid each reflux contains.
Treating GERD:
Drug therapy and lifestyle changes combine in the first stage of treating GERD. Several modifications particularly in how you eat and how you sleep have to be made. Those who experience heartburn are advised to sleep with their upper body elevated.
to sleep with their upper body elevated. This can be accomplished by sleeping with the upper body on a wedge or by tilting the bed. It’s worth noting that reflux also occurs less frequently when patients lie on their left rather than their right sides.
As for modifying your diet, begin by making your evening meals smaller and eating earlier. This will reduce the amount of reflux. Certain foods have been identified as promoting reflux by reducing the pressure in the lower esophageal sphincter.
Chocolate,
peppermint, alcohol, and caffeinated drink are on this list and should be avoided. Foods rich in fat should be reduced for the same reason, and smoking should be stopped all together.
When it comes to medication, antacids have long been the mainstay of those afflicted with heartburn. These work by neutralizing the acid in the stomach and reducing the acid in the reflux. Proton pump inhibitors and foam barriers are alternate drug treatments and are usually quite effective in treating the symptoms and complications of GERD.
However, in some patients they prove ineffective. Doctors consider surgery for such cases. Known as fundoplication, this surgery is very effective and offers great relief from the symptoms of GERD for several years. Nevertheless, many patients will continue to rely on drug therapy to cope with their reflux. |