There are different kinds of brain tumours, some which can be dealt with and cured, and others that will eventually kill you. Imagine a can of white paint; then imagine adding a few drops of black paint into this can - it disperses in the white paint, the concentration decreasing the further away one looks, from where the initial drop fell.
This is how a 'glioma', a brain tumour which arises from the brain tissue itself spreads. The borders are unclear like the drop of black paint as the tumour grows, and it is near impossible to remove it completely without leaving the patient with a significant disability.
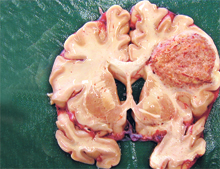 |
| Brain Tumour: Glioblastoma Multiforma |
'Gliomas' account for about 2% of all tumours that are diagnosed, so thankfully brain tumours are not common. But the impact on the patient and family from the time of diagnosis is tremendous. This is mainly due to the poor prognosis that they have. Gliomas do not spread to anywhere else in the body, like some other tumours such as lung cancer, but they are deadly.
The World Health Organisation has graded gliomas from I-IV. The higher the grade, the poorer the prognosis. The worst therefore is a Grade IV glioma, which is also called a Glioblastoma Multiforma.
In general, gliomas affect two age groups - those around 40-50 years and those above 65 years. The patient's age also has an impact on how he/she responds to treatment. The younger, fitter patient has a better chance of responding to the treatment compared to the latter group.
Males are affected more by gliomas than females. Generally they are not inherited. There have been no environmental factors or dietary factors that have proved to increase the chance of getting one of these tumours either. In short, nobody knows what triggers them to grow, yet.
Symptoms
Symptoms vary (as with anything within a closed cavity -the skull), as do the size of the tumours and the site. Patients may complain of early morning headaches, vomiting and fits. These symptoms may gradually worsen. When the tumours increase in size and infiltrate surrounding brain tissue, it may alter the function of the normal brain tissue and the functions it is involved in. Patients may present as if they had had a stroke. There maybe behavioural changes. Speech may be affected.
Signs
Again all signs of having an abnormal growth are within the skull. If the pressure within the skull is high, it maybe a condition called 'papilloedema' which will be seen by your doctor as he examines the back of your eye with a special tool called the ophthalmoscope. There may be weakness in the limbs, also problems in swallowing and speech.
Diagnosis
This can be done by a good clinician. A good history and thorough examination is essential. This is to come to the right diagnosis as well as to rule out other conditions that may give rise in a similar manner, such as stroke, seizures and infections. The doctor will then organise investigations to confirm the diagnosis.
Investigations
The first line of investigation is a CAT scan. This maybe followed by an MRI scan which gives further details. Routine blood tests are also carried out. To confirm that this may not have spread from elsewhere in the body a chest x-ray and PET scans are sometimes carried out, but not always as these tumours have specific characteristics that can be viewed on the scan.
Management
After the diagnosis, the patient is referred to a neurosurgeon who will assess the patient and decide on treatment. A few factors are considered - the patient's state of health and physiological condition, age, and neurological state. The scans are reviewed and discussed to decide the best management and also if surgery is considered for surgical planning.
Current evidence and guidelines suggest the best possible outcome for the patient is by removing as much tumour tissue as possible and then giving radiotherapy and chemotherapy. When the tumour is taken out, some tissue is sent to the lab to find out exactly what type of tumour it is and treatment adjusted accordingly.
As mentioned initially it is impossible to remove the tumour completely as the infiltration of the tumour may extend beyond the margins that we can see under a microscope. If the patient isn't in a good state of health and is not able to tolerate a lengthy operation, a biopsy is done. When this confirms the tumour grade, an individualised treatment regime is discussed and according to the patient's and family's wishes, treatment commenced.
Outcome
Unfortunately, even with the best treatment available, it only adds a maximum of a few months to the patient's life, if it is a glioblastoma multiforma. Generally most people die within a year. If the patient is diagnosed with a lower grade tumour, the length of survival is greater. Someone with a grade II glioma may survive for more than five years.
These are very nasty tumours, but the incidence is low and treatment is available. The good news is that there is a lot of research being carried out currently with promising initial results to increase the survival time of patients affected by these tumours.
|
