Many women will have ovarian cysts at some point in their lives, says Dr. Nalinda Rodrigo, consultant obstetrician and gynaecologist. While most will be harmless, and will disappear without treatment in a few months, some will rupture, and others might prove to be cancerous. Both conditions, if neglected, could escalate until they pose a serious threat to your health. This month he speaks to MediScene about the diagnosis and treatment of ovarian cysts.
What are ovarian cysts?
The fact is that many women will have ovarian cysts at some point in their reproductive lives - usually between the ages of 15 and 50. Women who are just past menopause are particularly vulnerable to cancerous cysts.
 |
| Courtesy nytimes.com |
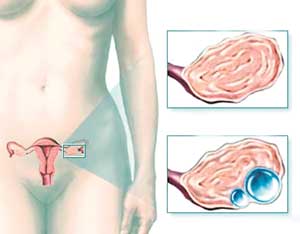
To place things in context, women have two ovaries - each about the size and shape of an almond - located on either side of their uterus. The ovaries develop and allow eggs or ova to mature, and ultimately release these eggs. This process results in the monthly cycle that women experience during their childbearing years.
Cysts are typically fluid-filled sacs within or on the surface of an ovary. Cyst-like structures called follicles commonly appear on ovaries each month. These follicles produce the hormones oestrogen and progesterone and also release an egg when you ovulate. Sometimes a normal monthly follicle just keeps growing. When that happens, it becomes known as a functional cyst. This means it started during the normal function of your menstrual cycle. It's worthwhile noting that cysts that appear in your ovary are not necessarily filled with fluid only. There can be a solid component or they can be entirely solid.
Types of Functional Cysts
There are two types of functional cysts:
Follicular cysts: Approximately at the midpoint of a menstrual cycle, the brain's pituitary gland releases a surge of luteinizing hormone (LH), which signals the follicle holding the egg to release it. When everything goes according to plan, the egg is released from the follicle and begins to move down the fallopian tube and towards possible fertilization.
However, when the LH surge doesn't occur, a follicle doesn't rupture or release its egg. Instead it grows until it turns into a cyst. These cysts are usually harmless, and they rarely cause pain, often disappearing on their own within two or three menstrual cycles.
Corpus luteum cyst: When LH surge does not occur and your egg is released, the ruptured follicle begins producing large quantities of oestrogen and progesterone in preparation for conception. This changed follicle is now known by the name of 'corpus luteum’. Sometimes, however, the opening through which the egg was released seals off and fluid begins to accumulate inside the follicle, causing the corpus luteum to expand into a cyst.
Although this cyst usually disappears on its own in a few weeks, it can grow to almost 5 inches in diameter. It may also bleed into itself or twist the ovary, resulting in pelvic or abdominal pain. If it fills with blood, the cyst may rupture, causing internal bleeding and sudden, sharp pain.
Symptoms
You may not even know that you have an ovarian cyst. In fact, it's highly possible that you will exhibit no symptoms at all. In such cases, the only chance of catching your cysts may be through a regular checkup.
However, if you have an ovarian cyst, you may very well experience some of these symptoms:
- Menstrual irregularities
- Pelvic pain - a constant or intermittent dull ache that may radiate to your lower back and thighs
- Pelvic pain shortly before your period begins or just before it ends
- Pelvic pain during intercourse (dyspareunia)
- Pain during bowel movements or pressure on your bowels
- Nausea, vomiting or breast tenderness similar to that experienced during pregnancy
- Fullness or heaviness in your abdomen
- Pressure on your rectum or bladder - difficulty emptying your bladder completely
The signs and symptoms that signal the need for immediate medical attention include:
- Sudden, severe abdominal or pelvic pain
- Pain accompanied by fever or vomiting
Screening and diagnosis
A cyst on your ovary may only be found during a routine pelvic exam. This is one reason why doctors recommend regular checkups - that include a trans-vaginal scan and pap smear - every five years for women over the age of 35.
To identify the type of cyst, your doctor may ask you to have a trans-vaginal or abdominal scan. If a cyst is suspected, doctors often advise further testing to determine its type and whether you need treatment and importantly whether cancer is a possibility. A CA 125 blood test allows doctors to measure the blood levels of a protein called cancer antigen 125 (CA 125.) These levels are often elevated in women with ovarian cancer. However, as elevated CA 125 levels can also occur in noncancerous conditions, such as endometriosis, it is not considered an infallible cancer marker.
Treatment
Treatment depends on your age, the type and size of your cyst, and your symptoms. Your doctor may suggest that you simply wait it out, until a re-examination in a few months. Birth control pills might be prescribed - these reduce the chance of new cysts developing in future menstrual cycles. Oral contraceptives also offer the added benefit of significantly reducing your risk of ovarian cancer - the risk decreases the longer you take birth control pills.
However if your cyst is very large, doesn't look like a functional cyst or persists through two or more menstrual cycles, your doctor might advise surgery. Cysts that cause pain or other symptoms may also need to be removed.
Some cysts can be removed without removing the ovary in a procedure known as a cystectomy. Your doctor may also suggest removing the affected ovary and leaving the other intact in a procedure known as oophorectomy.
Both procedures may allow the woman to maintain her fertility if she wishes to have children. Leaving at least one ovary intact also has the benefit of maintaining a source of estrogen production.
If a cystic mass is cancerous, however, a hysterectomy with removal of both ovaries and fallopian tubes may prove necessary.
| 