
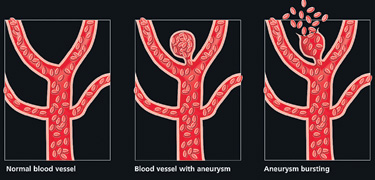
When the explosion is in your head"It was like an explosion in my head," said the patient who had just suffered from a brain haemorrhage (called Sub Arachnoid haemorrhage) coming in to the Neurosurgery Ward. This is not just any haemorrhage, this is a serious, life-threatening condition. Where is the haemorrhage or bleeding? There are three protective coverings over the brain. On the surface lies the pia mater, followed by the sub arachnoid mater and finally on the outside, the dura mater. The blood vessels supplying the brain lie in the layer between the pia and the sub arachnoid layer. Weak points in these vessels give rise to blisters or outpouchings of the vessels, which are called aneurysms. 2% of the population have these aneurysms, which are called berry aneurysms. Rupture of these aneurysms results in a sub arachnoid haemorrhage which is life threatening.
The sudden onset headache described by the patient is normally at the point at which this aneurysm ruptures. As the blood enters the water-like fluid circulating in the sub arachnoid space it irritates the membrane causing headache, neck pain and photophobia (where you cannot look directly into the light). The patient may also have a decreased level of consciousness, become drowsy and develop weakness of limbs. Sometimes the bleeding in the brain is more extensive: Fifty percent of patients who suffer from a sub arachnoid haemorrhage do not reach the hospital because the severity of the haemorrhage is fatal. What causes them? There are certain risk factors associated with sub arachnoid haemorrhage, such as smoking, high cholesterol, diabetes and high blood pressure. Presentation "It was as if someone hit me over the head with a bat", "worst headache of my life", "explosion in my head", are some of the descriptions given by patients. They may also say that the headache was associated with feeling sick and some even say they have vomited. Management The patient should be seen as an emergency by a medical team. A good history should be taken from the patient if he/ she is able to give one or if not from the relatives. Other causes of severe headaches should be ruled out, such as migraines. Sometimes this can be difficult and therefore they may need further tests to confirm what is wrong. After the patient has been stabilised then the initial investigation of choice is a Computerised Tomography scan (CT scan). Most of the time the scan will indicate a distinctive distribution of blood. There may even be a blood clot. On occasion the CT scan may not reveal any blood, but if the history is positive currently it is recommended that they have a further test called a lumbar puncture. This is where some fluid, which surrounds the brain and spinal cord, is taken for analysis by inserting a needle through the spine. If this test shows the presence of blood then a sub arachnoid haemorrhage is confirmed. The next test which the patient has when blood is detected by the scan or lumbar puncture is digital subtraction angiogram (DSA). This is where a dye is injected through a vessel in the groin and by taking multiple x-rays the whole brain's blood supply can be mapped out. This will show us where the abnormality is so that it can be treated. In the UK currently a specialised CT scan, which can also give us a map like this is also used but to date the gold standard test is an angiogram. Treatment The patient is started straightaway on fluids through a drip and kept on bed rest. Painkillers are given for the headaches as are anti-sickness tablets. A drug called Nimodipine is started, which helps to reduce the effects of narrowing of the blood vessels of the brain, which can happen after SAH. Narrowing of blood vessels can result in a stroke if not treated early. There are two treatment options - the traditional method, which has been proven to work well is to have a brain operation where the blister is identified and a clip is placed across its neck. This prevents it from bleeding again. This requires an operation and has its associated risks.
The other technique is done using the same method used to identify the blister - the angiogram. When the blister is identified, very fine platinum wires are passed through the vessels and the blister is packed with these to prevent further rupture. These wires are expensive and the number of wires required will depend on the size of the blister. The method also has complications but less so than a brain operation. After the treatment, the patient is kept in hospital for a further period till his/her condition stabilises. There are other problems that may arise along the recovery period so the patient will have further blood samples taken and scans. Constant attention is needed till recovery is made. Not all recover fully and they may be left with some degree of disability. Sub arachnoid haemorrhage can also occur due to other conditions but these are of less severity and are not discussed here. So if someone complains of a severe 'explosion' in their head always remember that it could be due to a ‘bomb’ in their brain. They need to be seen by the bomb squad at the closest hospital! (The writer is a Specialist Registrar in Neurosurgery in Manchester) |

|
||||||
|| Front
Page | News | Editorial | Columns | Sports | Plus | Financial
Times | International | Mirror | TV
Times | Funday
Times | Medi Scene || |
| |
Reproduction of articles permitted when used without any alterations to contents and a link to the source page.
|
© Copyright
2008 | Wijeya
Newspapers Ltd.Colombo. Sri Lanka. All Rights Reserved. |